Kyasanur Forest Disease(KFD): Indian Viral Hemorrhagic Fever
Introduction
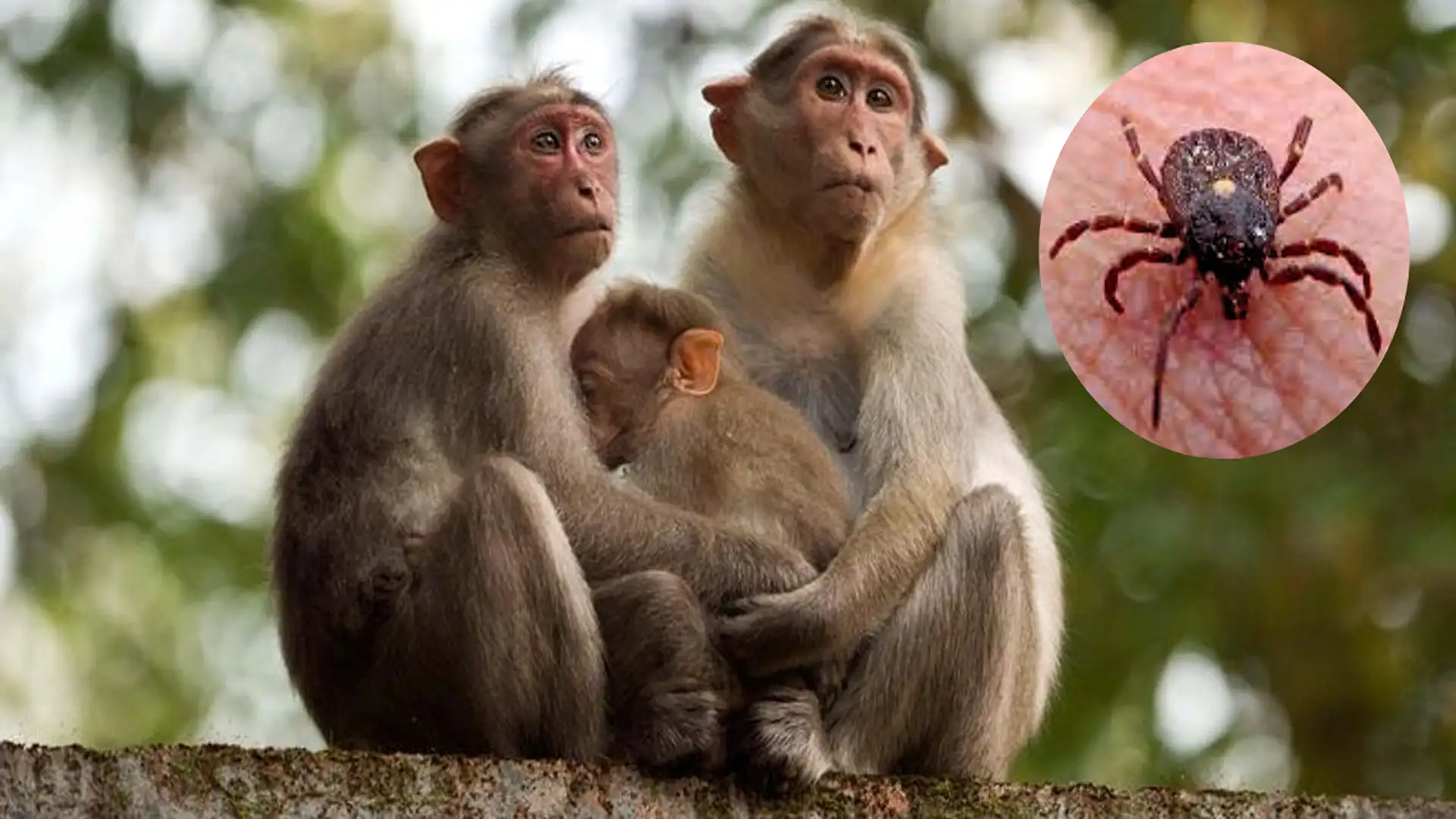
Kyasanur Forest Disease (KFD) is a viral hemorrhagic fever thatwas first identified in the Kyasanur forest range in Karnataka state in 1957.The disease is colloquially called “monkey disease or monkey fever”. KFD is largely confined to the southern Indian states of Karnataka, Tamilnadu, and Kerala along the western ghat ranges. At the same time, sporadic cases have been reported in Maharashtra and Goa. Annually nearly 400-500 people contract the disease. KFD can have a fatality of 3-10% and there is no specific treatment or cure.
Epidemiology & Transmission
The Kayasanur Forest Disease Virus (KFDV) belongs to the Flaviviridae family and is transmitted by an arthropod (ticks). It is a zoonotic disease transmitted by ticks Haemaphysalisspinigera from rodent reservoirs (rats, shrews, squirrels) in the forest. Non-human primates (monkeys) act as an amplifying host. Monkeys become ill after being bitten byvirus-infested ticks while foraging for food on the forest floor, most of these primates die due to heavy viremia. An outbreak of KFD in monkeys (Epizootic) can lead to a spillover event in the human population in the surrounding area. When humans are bitten by aKFDV-infested tick or infected animal transmission can happen.
Clinical Manifestations & Mortality
The incubation of the disease is roughly a week (7-9 days), followed by bleeding, skin eruptions, chills, rigors, fever, malaise, heart and brain complications, red eye, change in blood picture, altered sensorium, organ dysfunctions, dehydration and circulatory collapse, coma, and death. The mortality is around 3% but it can reach 10% depending on the strain and host conditions. As it’s a viral hemorrhagic fever, KFD patients need to be treated in facilities with biosafety and insect control. This can be a problem in an outbreak setting where there can be a surge in hospitalization.
The diagnosis is largely clinical based on symptoms of bleeding and a strong travel history to the Kyansanur forest area. However, confirmation can be done by ELISA IgM,RT PCR, or Rapid Nucleic Acid Testing devices.
High Risk Groups
Ecotourist
s
/Hikers/Trekkers
Wildlife
Biologists/
Photographers
Forest
Officials/
Conservationist
s
Wildlife Veterinarians
/Rangers
Primate Handlers
/Researchers
Animal
Hunters/
Firewood Gatherers
Fruit
&
Nut
Farmers/
Harvesters
Villagers/Tribal Communities
Global Health Implications
In the past KFD has been geographically limited to Kyasanur forest and its adjoining areas. However, in 1989-90 fifty or more cases were reported in Yunnan province of China. Migratory birds carrying infested ticks have been implicated in KFD appearing in distant geographic locations. This observation has huge implications for global health. KFD has the potential for worldwidespread due to the transnational movement of tick-infested migratory birds. Meanwhile, KFDV is a level 4 biosafety pathogen and has to be handled in appropriate containment facilities.
Management & Prevention
In the absence of specific antiviral therapy, only supportive care is possible.Since KFD is a hemorrhagic fever excessive bleeding from various sites is expected. Apart from thatorgan dysfunctions, intravascular clotting, dehydration, and circulatory collapse are other complications. Maintenance of hydration, transfusion of blood and blood products, and prevention of secondary infections are key to survival. Cardiac and neurological complications are seen in the late phase of the disease. People in the extremes of age and co-morbidities will have higher mortality rates. Few antivirals are being screened by computational methods and few others are being repurposed (Favipiravir, Sofosbuvir, Nitazoxanide, mAbTyzivumab), still, none of them have been proven to improve survival.
A formalin-inactivated tissue culture two-dose vaccine is currently available. During an outbreak, immunization is carried out in populations living within a 6 km radius of the index cases. Foresters and individuals venturing into the Kayasanur forest zone are recommended for vaccination.A newer vaccine for KFD is also under development at the time of this writing.
Using insect repellents like ( DEET) and wearing long sleeves, gumboots and avoidance of tick bites are some of the preventive measures. Frequent visitors to the Kyasanur forest zone can get vaccinated. Avoiding dead monkeys and animal carcasses in the forest is important, as ticks can leave dead monkeys and search for alternate hosts.
Similarly, environmental control withlarge-scale insecticide spraying, and de-ticking cattle and pet animals. Routine administration of ivermectin to animals, and de-ticking baths are some of the disease control measures. However, these are quite impractical and may not be applicable on a routine basis.
Conclusion
KFD is an emerging tropical disease of national and global importance. It also has implications for travel medicine. High-risk groups like tourists, forest visitors, local communities, and adventure enthusiasts should be awareof the dangers of this fatal viral disease. Even with effectiveantivirals and biologicals in the future, prevention will always remain indispensable.
Gifty Immanuel MD,PhD, FRCP,FIDSA
References
Douglas D. Richman. (4th ed.). Clinical Virology fourth edition. American Society of Microbiology (2016).
Firth, John, Christopher Conlon, and Timothy Cox (eds), Oxford Textbook of Medicine, (6th ed) (Oxford, 2020).
Mandell Douglas and Bennett’s Principles and Practice of Infectious Diseases (9th ed). Elsevier (2020).